
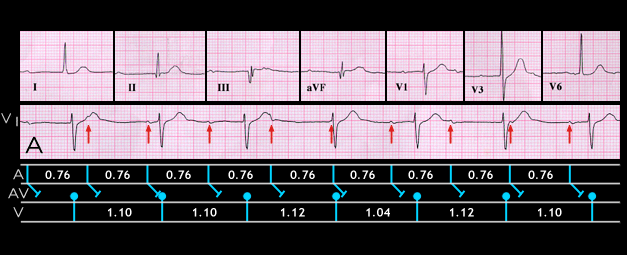
The ECGs shown here and on the next several pages illustrate the variable and transient nature of the AV conduction disturbances that are associated with an inferior wall infarction. This ECG, labeled “A”, shows complete AV block with an AV nodal escape rhythm. It was recorded from a 47 year old male following an episode of lightheadedness but without significant chest pain. The atrial rate is 80, the ventricular rate is 55 and there is AV dissociation. The P waves, although small, are best seen in lead V1 (arrows) and appear normal. The QRS complexes show a Q wave in leads II, III and aVF and slight ST elevation in leads III and aVF, suggesting a recent inferior wall myocardial infarction. The cardiac enzymes were elevated consistent with an infarction occurring within 48 hours of the tracing.