
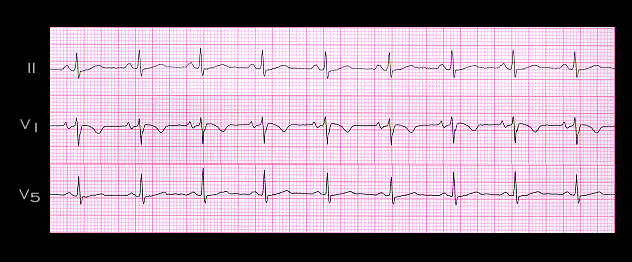
This tracing, from the same patient, was recorded shortly after the intravenous administration of adenosine. There is now sinus rhythm with a rate of 80 per minute and a PR interval of approximately 0.16 seconds. The deflection suggestive of an R’ in V1 is no longer present, confirming that it was caused by a retrograde P wave. The ST segment depression seen in leads II and V5 during the tachycardia is also no longer present. This could also have been a manifestation of the retrograde P wave, or an indication of ischemia induced by the sudden increase in rate. The presence of the retrograde P wave in or beyond the end of the QRS complex is consistent with the retrograde pathways being either within the AV node and perinodal tissue, or in an AV nodal bypass tract. In general, the more displaced the retrograde P wave from the end of the QRS complex, the more likely it is that an AV nodal bypass tract formed the retrograde limb of the re-entry circuit