
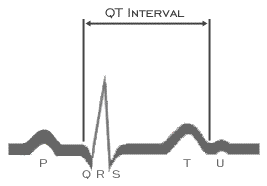
The QT interval is measured from the earliest onset of the QRS complex to the latest end of the T wave. It represents the interval from the onset of ventricular depolarization (the beginning of QRS complex) to the end of ventricular repolarization (the end of the T wave), and assumes we are capable of accurately detecting both of these points from the 12 lead body surface ECG and that there is no depolarization or repolarization that not represented on the 12 lead body surface ECG, i.e, is "silent". It is important to remember that The QT interval varies in the various leads because of the varying relationship of the components of the ECG waveform to the lead axis. This variability is particularly prominent in the limb leads. When measured manually, the lead with the longest QT interval should be used. This is most often Lead V2 or V3. The measurement performed by automated ECG machines is done from superimposed median beats. This allows detection of the earliest QRS onset and latest T wave end and may be as much as 20 ms longer than that measured in any individual lead. In addition, the QT interval varies with gender (it is slightly longer in females than in males) and time of day, being longer in the evening. For these reasons, it is difficult to identify a normal value. Most investigators agree that an upper limit of 440-450 ms is appropriate, but the range of normal values is wide.
The QT interval also varies as a function of rate, being shorter at more rapid rates and longer at the slower rates. This rate dependency is discussed on the next several pages