
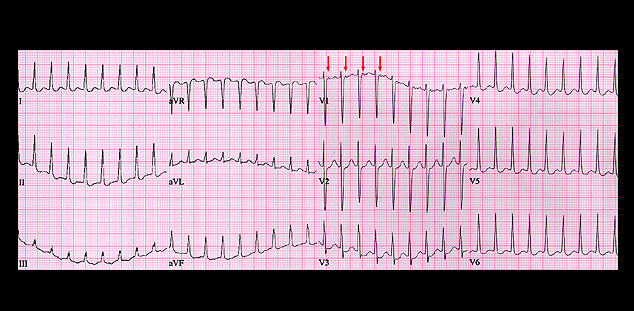
The rhythm is regular with a rate of 210. There are several possible interpretations of this tracing. The rate is more rapid than usual for either sinus tachycardia or atrial flutter with 2:1 AV block, but the possibility of slow atrial flutter with 1:1 conduction can not be excluded. Note that there is a very subtle deflection at the end of the QRS complex (or in the early portion of the ST segment) that is seen best in leads V1 and V2 (red arrows). This may be a P wave and if so, could be the P wave of an ectopic atrial tachycardia. However, the more likely diagnosis is an AV junctional reentrant tachycardia. The presence of the P wave at the end of the QRS complex suggests that the retrograde limb of the reentrant pathway is outside of the AV node and represents an AV nodal bypass tract.