
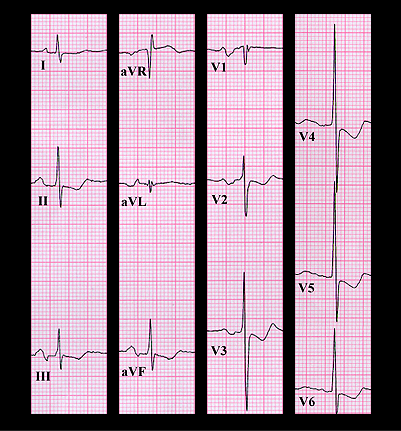
Her ECG shows sinus rhythm with a PR interval that is at the upper limit of normal (about 0.20 seconds). The P waves suggest left atrial enlargement (P mitrale) and the frontal plane axis is normal (+69 degrees). The small S wave in lead V1 is consistent with right ventricular hypertrophy while the deep S wave in lead V3 and the tall R waves in leads V4 and V5 are consistent with left ventricular hypertrophy. There are also ST segment and T wave changes that could be due to the hypertrophy and/or to digitalis. This constellation of ECG and physical findings suggests biventricular hypertrophy due to the combination of mitral stenosis, mitral insufficiency and pulmonary hypertension. The prominent ”v“ waves observed in her neck veins suggests that the systolic murmur may also have contained a component caused by tricuspid insufficiency. These diagnoses were confirmed by further studies.