
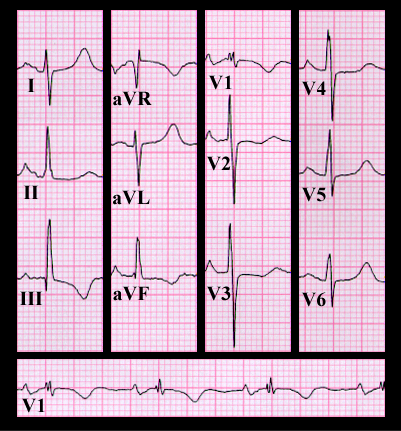
Her ECG, shown again here, reveals sinus rhythm with a normal PR interval and normal QRS duration. The frontal plane spatial vector is directed inferiorly and slightly to the right (as in the prior patient whose ECG was shown on page 9.1.27) with an axis of +100 degrees. However, in this patient, the P waves are broad and notched in leads I, II, aVL with a prominent negative component in lead V1. Thesse P wave findings are referred to as "P mitrale" amd suggest left atrial enlargement or an intra-atrial conduction delay. In addition, the S wave in lead V1 is very small and the R and S wave amplitudes in lead V6 are equal. These changes, and the right axis deviation, suggest right ventricular hypertrophy.
The ECG changes suggestive of left atrial enlargement and right ventricular hypertrophy, in combination with the auscultatory findingsdescribed here, are virtually diagnostic of mitral stenosis with moderate pulmonary hypertension. This was the diagnosis in this patient. A 10 mm Hg pressure gradient was present across her mitral valve during diastole. Her pulmonary artery systolic pressure was 37 mm Hg at rest and increased to 60 mm Hg with mild leg exercise performed during the catheterization.
Although acute rheumatic fever with subsequent mitral and aortic valvular disease has become much less common in the United States and other industrialized nations, it remains a major health problem in less well developed regions of the world.