
[IF POSSIBLE,INSERT ARROWS TO P WAVES IN LEADS V4-6]
They also noted that while AV dissociation was highly specific for ventricular tachycardia, retrograde conduction to the atria, i.e.VA conduction, providing an association between the ventricular and atrial complexes, also occurred commonly in patients with idioventricular rhythms and ventricular tachycardia.
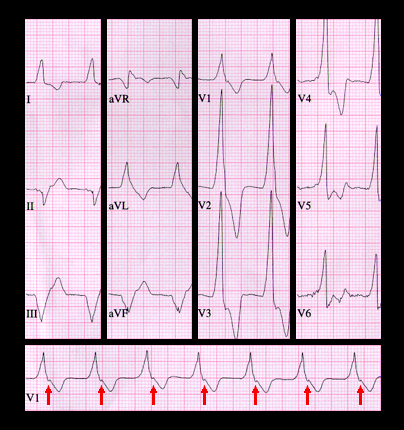
The ECG displayed here is from an 18 year old female with no known heart disease. It shows a wide complex rhythm with a rate of 94 and a QRS duration of 0.18 seconds. The QRS morphology suggests right bundle branch block with a superior frontal plane axis and a single positive (upright) component in lead V1, indicative of it being ventricular in origin. There are no P waves preceding the QRS complex and no AV dissociation, but there is a deflection at the beginning of the ST segment, seen best in leads V1 and leads V4, V5 and V6 (arrows), caused by a retrograde P wave indicating 1:1 VA conduction. This is an example of an accelerated idioventricular rhythm (or slow ventricular tachycardia) with retrograde VA conduction.